
Thyroid health: If you only do the conventional blood tests, you might miss something
- Marie Perez FNTP, HINT, MSTAT

- Dec 8, 2025
- 5 min read
If you find yourself suffering from:
Cold hands and feet
General sensitivity to the cold
Abnormal hair loss
Losing the outer third of your eyebrows
Low energy, feeling generally sluggish
Gaining weight
Constipation
Dry skin, cracked heels, thickening skin and nails
Rising cholesterol when you get your blood tested
Feeling anxious

…then your doctor may well suggest you get a thyroid blood test – they will be thinking that you may be suffering from hypothyroidism, or an under-active thyroid. These are some classic symptoms.
In conventional medicine, the 2 blood markers that are generally tested are:
TSH (thyroid stimulating hormone) and
free T4 (thyroid hormone thyroxine, unbound from its protein carrier).
So let’s break this down a bit. The thyroid is the butterfly shaped gland in your throat which controls the speed at which things happen – it’s like the gas pedal.

The thyroid is governed by the HPT axis, which stands for hypothalamus- pituitary-thyroid axis. The hypothalamus in the brain is like a thermostat, constantly monitoring the blood for levels of thyroid hormone. It signals to the pituitary when more thyroid hormone is needed, which in turn signals to the thyroid via TSH – thyroid stimulating hormone. The higher TSH, the louder the pituitary is “shouting” at the thyroid to make hormones.
T4 (thyroxine) is the main thyroid hormone produced by the gland, though it does make small amounts of T3 (tri-iodothyronine). T4 is release from the thyroid and then transported around the body in the bloodstream to then enter cells via receptors.
T3 is the active form which enters the cells. Conversion from T4 to T3 takes place peripherally – in other words in other parts of the body, not the thyroid – predominantly in the liver, kidneys and muscles.
You may already be asking the question …. But if T3 is the active form, why ae we only testing for T4? Great question! Here are some other things to consider.
Thyroid hormone can’t just be allowed to float round in the blood stream as it is, it needs to be bound – in this case, in a specialised protein called TBG (thyroxine binding globulin). It is released from this protein when needed, hence “free T3” and “free t4”.
Unfortunately the thyroid gland seems to be particularly susceptible to “friendly fire” or being attacked by our body’s own immune system – this autoimmune disease is called Hashimoto’s. When this happens there are antibodies that are produced – the 2 main ones are thyroid peroxidase (TPO Ab) antibody, and the other thyroglobulin antibody (or TGAb)
And a third thing…bear with me here because I find this one fascinating. Remember that thyroid hormone is like your accelerator pedal. If your body perceives that you need to ease off the gas for any reason, e.g. because you are ill, because your adrenals are saying woah too much going on here, or because there is a famine (unlikely these days I. know), or anorexia, or some other reason, your body will slow you down by messing with the structure of your T3, remember, this is your active hormone, and instead make REVERSE T3.
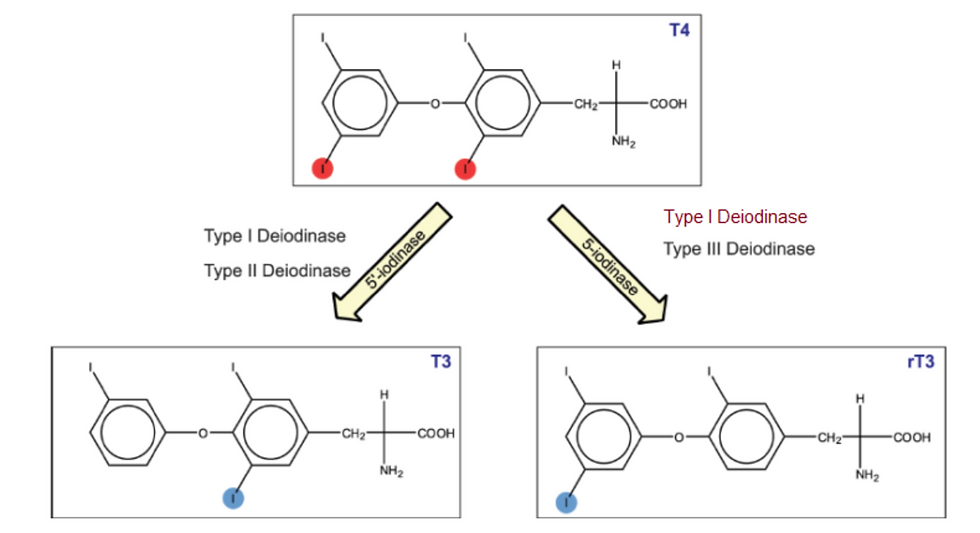
When T4 is converted to T3, all that happens is that one iodine “arm” is removed from the T4 molecule (the enzyme that does this is called de-iodine-ase – see? It "de-iodines" the T4 by one iodine). But when your body is trying to slow you down it will remove the WRONG arm, creating a molecule that will no longer pass through the T3 receptor, meaning the hormone is not delivered to your cell nucleus….and you have been effectively slowed down.
So, big breath, these are reasons why, on a full thyroid panel (like the one I run on my clients) you will see all these markers:
TSH – your brain telling your thyroid to make more hormone (conventional marker tested)
Free T4 – the inactive hormone unbound from its protein carrier (conventional marker tested)
Free T3 – the active hormone unbound from its protein carrier
T4 – total amount of inactive hormone, bound and unbound
T3 - total amount of active hormone, bound and unbound
Reverse T3 – T3 that has been molecularly altered to “not work”
TPO Ab – antibodies against your thyroid
TG Ab – another type of antibody against your thyroid
That is 8 – yes 8 – markers that are tested, not just the first 2. Why is this important?
In recent weeks I have had 3 clients, all female, run full thyroid panels like the one above. In 2 of those cases the conventional approach of running just the first 2 markers ….the clients’ results fell within the normal ranges and they would have been told all is well, bye bye. BUT the more extended panel revealed something else. I’ve set this out below:
Case 1: TSH high (but within normal reference range), free T4 a little low (but also within reference range). BUT free T3? Low. This client was a mum to 2, also working as a teacher and SENCO, and had previously had part of her thyroid removed. The basic issue was that she was not quite making enough T4, and conversion of that T4 to T3 wasn’t great. Conversion needs a certain set of nutrients to be present - notably selenium and zinc - but can also be suboptimal when a client has been “giving a lot” for a long time.
Case 2: Perfect TSH, perfect free T4, BUT low free T3 AND slightly elevated TPO antibodies. This client had been diagnosed with Hashimoto’s several years previously and was generally managing it well – her antibodies were only just out of range. But the issue here again was the low T3 – she wasn’t converting well. Again, this would not have been picked up if a standard thyroid test of just TSH and free T4 was run. Also note the Hashimoto’s – she is potentially running on less thyroid output than someone without Hashimoto’s as in episodes of autoimmune “attack” thyroid cells can be destroyed.
Case 3: TSH – a little high, outside of conventional reference range. Free T4 – perfect. But in this case, she tested the antibodies and while TgAb was normal, her thyroid peroxidase was greater than 1300. So in this case, a new diagnosis of Hashimoto’s disease.
This last case was interesting, for a number of reasons. There was a familial tendency to thyroid inflammation (both her mother and her grandmother has some form of thyroid disease). The client came for help initially with a form of exceptionally high anxiety…and this can be a symptom of the high antibodies present in Hashimoto’s.
So the main point I want to make is that if you only test TSH (remember, the pituitary to thyroid signal to make more hormone) and free T4 (inactive hormone) then you will likely miss a big part of the thyroid picture. With a conventional approach, clients 1 and 2 would have carried don as they were, unaware that they were not converting well to T3, the active hormone.
Thyroid health is a little complex but there are many things that can help to balance things out. BUT it all depends on the whole picture of the client. The other thing to bear in mind is that the thyroid does not just suddenly decide overnight to stop or slow down its hormone production, or to put the brakes on you by making reverse T3 instead of T3. This will have been going on for a while. Some questions I might ask clients are, in which area of your life are you giving too much, and why? What do you do to refill your tank – do you give yourself permission to e.g. do nothing for half an hour every day? Or maybe, have you recently moved towards perimenopause? Because unfortunately thyroid issues can raise their head at this life stage.
Phew. Quite a thyroid rollercoaster there! As I say, it’s a little complex but any questions, thoughts, queries, comments, please do reach out.
Wishing you all a peaceful festive season. Marie




Comments